Rural mental health poses a major challenge to our healthcare system. About 20% of Americans live in rural areas, and a fifth of them—roughly 6.5 million people—struggle with mental illness. The need for care is huge, but appropriate services remain hard to find. More than 150 million Americans live where mental health providers, especially psychiatrists, are scarce.
The numbers paint an even bleaker picture. Rural Americans face a severe shortage of mental health providers, with over 60% living in areas lacking adequate coverage. Nearly 65% of counties outside metropolitan areas don’t have psychiatrists. Rural communities also struggle with long travel distances to reach available providers. These challenges have led to a growing gap in mental health care needs. The number of people unable to access needed services jumped from 4.3 million in 1997 to 7.2 million by 2010.
This piece looks at how Community Access Programs (CAPs) help bridge these gaps and build stronger mental health support systems where they’re needed most. We’ll get into their role in mental health services, tackle the various obstacles they face, and see how they fit into broader healthcare policies.
Understanding the Role of CAPs in Mental Health Infrastructure
Community Access Programs (CAPs) play a vital role in mental health infrastructure. They act as bridges that connect vulnerable populations with essential care. Unlike traditional facility-based psychiatric services, CAPs build multi-sector partnerships, make community members central to interventions, and provide services in local community settings.
CAPs draw their strength from their community-based approach. These programs see mental illness as more than just an isolated issue – it’s a complex challenge that needs well-rounded solutions. They operate beyond conventional healthcare facilities and reach people in their homes, schools, community centers, and through technology platforms. This approach helps overcome common barriers like distance and transportation that often keep people from getting care.
These programs are changing how mental health services reach people. They bring together community health workers and peer support specialists with psychiatrists and psychologists. The programs use community settings where people feel more comfortable seeking help, with less fear of stigma. They work at different social levels to address individual needs as well as family, interpersonal, and institutional factors.
The financial approach of these programs makes mental health care available to more people. Many CAPs offer free or subsidized services because they know cost often stops underserved populations from getting help. This strategy has shown clear benefits: people’s quality of life improves, they become more physically active, face lower risks of homelessness, and need fewer stays in behavioral health hospitals.
CAPs have revolutionized mental health care by moving from institution-based to person-centered approaches. They bring services to where people live instead of making them find their way through complex healthcare systems. This approach works particularly well in rural areas where specialty mental health services are scarce and stigma often stops people from seeking professional help.
Multilevel Barriers CAPs Are Designed to Overcome
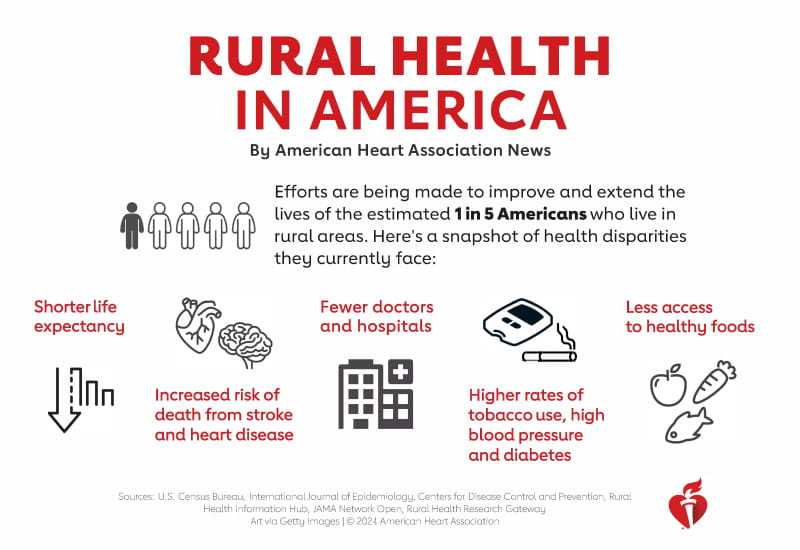
Image Source: American Heart Association
Mental health services in underserved areas face multiple barriers. These challenges create a complex web that CAPs need to address. Traditional healthcare models don’t work well in these communities, and understanding why helps explain the shortfall.
The nationwide shortage of available services remains a pressing concern. More than one-third of Americans (122 million) live in designated Mental Health Professional Shortage Areas. Rural areas suffer the most. These counties show alarming statistics – 65% have no psychiatrists, while 81% lack psychiatric nurse practitioners. Rural patients must travel much longer distances to get care. They drive an average of 26.2 minutes to any mental health facility and 64.3 minutes to outpatient facilities.
Access to care presents another major hurdle. People without reliable transportation are 44% more likely to delay care, which affects how well they stick to treatment. Insurance coverage adds another layer of difficulty. Less than half of psychiatrists (46%) accept Medicaid. Many providers need payment right away because reimbursement rates are so low.
Stigma creates powerful psychological barriers, especially in terms of acceptance. Rural communities tend to value self-reliance. Small towns’ lack of privacy makes mental health care seeking risky for someone’s social status. Cultural beliefs also shape how people view and treat disorders. Some communities see these conditions as personal weaknesses rather than medical problems.
CAPs tackle these connected barriers through comprehensive approaches that match each community’s needs.
Policy Integration and System-Level Impact of CAPs

Image Source: Rural Health Information Hub
Federal, state, and local policy frameworks now recognize CAPs as vital parts of detailed mental health systems. Medicaid stands as the single largest payer for mental health services in the United States and has taken on a bigger role in substance use disorder reimbursement. This financial support helps many CAPs provide long-term services to vulnerable populations.
The Mental Health Parity and Addiction Equity Act has made healthcare more accessible by making sure mental health coverage matches medical benefits, which helps millions of Medicaid beneficiaries. States have also created new funding approaches. Indiana’s Adult Mental Health Habilitation program now provides home and community-based services to adults with serious mental illness.
Mental health services work best when they combine with primary care at the system level. Child and Adolescent Psychiatrists (CAPs) are in short supply – states like West Virginia have just 10 CAPs per 100,000 children. Primary care providers and behavioral health clinicians now work together to fill this gap. Research shows that combination therapy with medication and psychotherapy works twice as well for treating adolescent mental health disorders compared to using either method alone.
The federal government recently invested $1.50 billion to improve the 988 Suicide & Crisis Lifeline. This service received 469,023 contacts in May 2023. Significant challenges remain though. The pandemic affected 53% of rural adults’ mental health, and 37 million rural Americans still live in areas without enough mental health professionals.
Conclusion
Community Access Programs are crucial solutions to mental health challenges that rural America faces today. This piece shows how CAPs help bridge the substantial gaps in mental health care delivery. They work directly within communities instead of asking patients to traverse complex healthcare systems. These programs are changing care delivery through their community-based approach, strategic collaborations, and focus on making care accessible.
Traditional mental health infrastructure doesn’t serve millions of Americans well, especially those in rural areas. Data shows that more than 60% of rural Americans live in designated provider shortage areas. About 65% of nonmetropolitan counties have no psychiatrists at all. CAPs tackle these challenges by reaching people in their homes, schools, and community centers. This approach helps overcome geographical, financial, and cultural barriers.
On top of that, CAPs work at multiple levels to curb stigma, which often stops people from seeking help in close-knit rural communities. Their person-centered approach is different from institution-based care. This makes their services more acceptable to people who usually hesitate to get involved with formal mental health systems.
Policy frameworks now acknowledge these programs’ vital role. Medicaid has become the largest payer for mental health services. States have created innovative financing mechanisms that support community-based interventions. Yet, there’s still work to be done to merge CAPs into broader healthcare systems.
Looking at the future of mental health care in underserved areas, CAPs show a promising way forward. Their comprehensive approach improves individual outcomes and strengthens communities as a whole. We need to keep supporting these programs through steady funding, policy development, and research that proves they work. We can ensure all Americans have access to mental health support they deserve, whatever their location.
Key Takeaways
Community Access Programs (CAPs) represent a transformative approach to addressing the mental health crisis in underserved areas, where over 60% of rural Americans live in provider shortage areas and 65% of nonmetropolitan counties lack psychiatrists.
• CAPs bridge critical gaps by delivering mental health services directly in communities—homes, schools, centers—rather than requiring travel to distant facilities.
• Multi-barrier approach works: CAPs simultaneously address provider shortages, insurance gaps, transportation issues, and cultural stigma through community-based partnerships.
• Policy integration accelerates impact: Medicaid funding and federal investments like the $1.5 billion for 988 Crisis Lifeline enable CAPs to provide sustained, accessible care.
• Person-centered care reduces stigma: By operating outside traditional healthcare facilities and using peer support specialists, CAPs make mental health services more acceptable to reluctant populations.
• Collaborative models prove effective: Integration with primary care and combination therapy approaches show significantly better outcomes than single-intervention strategies.
The success of CAPs demonstrates that effective mental health care requires meeting people where they are, not where systems expect them to be. This community-first approach offers a scalable solution for the 37 million rural Americans still living in mental health professional shortage areas.
FAQs
Q1. What are Community Access Programs (CAPs) and how do they improve mental health support? Community Access Programs are initiatives that bring mental health services directly to underserved communities. They operate in homes, schools, and community centers, making care more accessible and reducing barriers like transportation issues and stigma.
Q2. How do CAPs address the shortage of mental health providers in rural areas? CAPs employ a diverse team of professionals, including community health workers and peer support specialists, alongside traditional providers. This approach helps overcome the severe shortage of psychiatrists and other mental health professionals in rural counties.
Q3. What role does Medicaid play in supporting Community Access Programs? Medicaid is the largest payer for mental health services in the United States. It provides crucial financial support that enables many CAPs to offer sustained services to vulnerable populations in underserved areas.
Q4. How do CAPs help reduce the stigma associated with seeking mental health care? By operating in familiar community settings and utilizing peer support specialists, CAPs create a less intimidating environment for seeking help. This approach is particularly effective in rural communities where stigma can be a significant barrier to accessing mental health services.
Q5. What impact have CAPs shown in improving mental health outcomes? CAPs have demonstrated measurable benefits, including improved health-related quality of life, increased physical activity, reduced homelessness risk factors, and decreased behavioral health hospitalizations. Their community-based approach has proven especially valuable in rural areas where specialty mental health services are scarce.